Advanced Practice Provider Utilization and Compensation | Case Study
Optimizing advanced practice provider utilization to increase retention and engagement
Featuring a case study from a large academic medical center
DOWNLOAD FULL ARTICLE
At a time when healthcare organizations remain focused on pandemic-related financial and care delivery challenges, there is an acute need to engage and retain the clinical workforce by reducing burnout and unexpected turnover – and how advanced practice provider utilization within the care team can have a significant impact on both.
As organizations look for better ways to support their growing APP workforce, they require an intentional approach that aligns compensation design more closely with the goals of care team optimization in order to reduce costs and improve team performance.
In an article written by SullivanCotter and published by the American Association of Provider Compensation Professionals, learn more about how one organization set the stage for optimal APP utilization and care team delivery by also addressing important compensation issues at the same time.

PRESS RELEASE | SullivanCotter Names New Independent Members to its Board of Directors
New Independent Directors will play a pivotal role in providing the additional insight, experience and external perspective needed to support business strategy, ensure organizational growth and maintain independence
May 18, 2021 – Chicago –SullivanCotter, the nation’s leading independent consulting firm in the assessment and development of total rewards programs, workforce solutions, and technology and data products for the health care industry and not-for-profit sector, is pleased to announce the addition of five independent advisors to the firm’s Board of Directors.
“While our firm continues to expand and evolve amidst a number of unprecedented industry changes, advancing our strategic plan to help better serve the dynamic and unique needs of our clients remains a top priority. By inviting an accomplished group of Independent Directors to join our Board, we hope to leverage their strategic thinking, market knowledge and many years of combined experience as we move forward into 2021 and beyond,” said Ted Chien, President and CEO, SullivanCotter.
In an effort to prioritize best practices in governance, information technology, financial and human capital development, and diversity, equity and inclusion, SullivanCotter welcomes the following Independent Directors to the Board:
- Gina Alexander – Current Chief Financial Officer for AlixaRx, a privately-held, technology-enabled pharmacy services company serving the long-term care and corrections market.
- Brian Dunn – An experienced consultant who retired as the Chairman of McLagan and the CEO of Performance, Reward and Talent at Aon Consulting.
- Frances Ferguson – An accomplished C-Suite executive with more than 25 years of experience who most recently served as Group Executive, Managing Director and the Chief Administrative Officer of the Financial Markets and Treasury Services Sector operations at BNY Mellon Bank.
- Paul Keckley – Managing Editor of The Keckley Report, a health care policy analyst and widely known industry expert who advises health care organizations on long-term growth, sustainability, and advocacy strategies.
- Robert Oberrender – A decorated financial executive who recently retired as the Chief Investment Officer and Treasurer of UnitedHealth Group in October 2018.
As SullivanCotter continues to innovate through its performance-focused advisory services and growing suite of technology, survey and data products, these new members will play a pivotal role in providing the additional insight, experience and external perspective needed to support business strategy, ensure organizational growth and maintain independence.
To learn more about SullivanCotter’s Board of Directors, visit us at SullivanCotter.com or call 888.739.7039.
About SullivanCotter
SullivanCotter partners with health care and other not-for-profit organizations to understand what drives performance and improve outcomes through the development and implementation of integrated workforce strategies. Using our time-tested methodologies and industry-leading research and information, we provide data-driven insights, expertise, data and technology to help organizations align business strategy and performance objectives – enabling our clients to deliver on their mission, vision and values.
READ ON NEWSDIRECT

PRESS RELEASE | SullivanCotter Welcomes Information Security Officer Jeff Peal
Ensuring client-facing solutions remain highly effective, secure and compliant
April 27, 2021 – Chicago –SullivanCotter, the nation’s leading independent consulting firm in the assessment and development of total rewards programs, workforce solutions, and technology and data products for the health care industry and not-for-profit sector, is pleased to announce the addition of Jeffery A. Peal as its Information Security Officer.
With over 20 years of cybersecurity and information technology experience, Jeff has a longstanding passion for providing business-enabled solutions while also managing risk and strengthening organizational security. His demonstrated ability to envision, lead and implement innovative IT programs helps to enhance security awareness, increase productivity, and mitigate risk and exposure.
“Now more than ever, the not-for-profit and health care industry continues to transform its information security practices at a rapid pace. As our clients look to stay ahead of the curve in an increasingly complex environment, SullivanCotter continues to innovate through its growing suite of technology, survey and data products. With Jeff’s specialized knowledge and expertise in business intelligence, data and information security, he will play a pivotal role in our risk-based approach to ensure the firm’s client-facing technology solutions remain highly effective, secure and compliant,” said David Schwietz, Chief Information Officer.
Jeff works closely with clients to support compliance and assist with the way data is secured, managed and stored. He also directs SullivanCotter’s information security growth initiatives and resources internally to help drive greater value for clients. This includes establishing enterprise-level security initiatives, leading high-performing teams across a number of technical and analytical support areas, designing strategic information security policies, and auditing software and application vulnerability.
Prior to joining SullivanCotter, Jeff spent more than 20 years with the Federal Reserve Bank of Minneapolis where he most recently served as the Information Security Officer.
He also works as an adjunct professor and community faculty member at two Minneapolis-based technical colleges and universities to support higher education in information security and expand and develop local talent in this field.
About SullivanCotter
SullivanCotter partners with health care and other not-for-profit organizations to understand what drives performance and improve outcomes through the development and implementation of integrated workforce strategies. Using our time-tested methodologies and industry-leading research and information, we provide data-driven insights, expertise, data and technology to help organizations align business strategy and performance objectives – enabling our clients to deliver on their mission, vision and values.
READ ON NEWSDIRECT

PRESS RELEASE | Benchmarks360™ - APP Utilization and Perceptions Manager
SullivanCotter Releases Comprehensive APP Utilization and Perceptions Manager for its Growing Benchmarks360™ Platform
April 21, 2021 – Chicago – SullivanCotter, the nation’s leading independent consulting firm in the assessment and development of total rewards programs, workforce solutions, and technology and data products for the health care industry and not-for-profit sector, is pleased to announce the addition of powerful new capabilities for assessing advanced practice provider (APP) utilization and workforce perceptions to its growing Benchmarks360™ platform.
Powered by SullivanCotter’s proprietary surveys and research, Benchmarks360™ is a suite of intelligent, web-based products that enables health care organizations to analyze and visualize compensation, clinical productivity and workforce perceptions through industry-leading data, analyses and reporting.
"In today's unprecedented health care environment, it is important for organizations to utilize, engage and retain their clinical workforce more effectively. APP turnover can significantly impact cost, morale and operations, and gaining access to the right data and benchmarking tools can help to enhance workforce retention, team-based care practices and organizational performance during such a critical time,” said Amy Noecker, APP Workforce Practice Leader, SullivanCotter.
SullivanCotter’s Benchmarks360™ APP Utilization and Perceptions Manager allows organizations to collect, benchmark and report on the thoughts and experiences of their APPs and physicians related to APP compensation, resources and job responsibilities to help ensure current pay programs and care models are competitive and effective. In addition to data on nurse practitioners and physician assistants, it also provides information and analysis on other members of the APP workforce including certified registered nurse anesthetists and certified nurse midwives.
This new module includes two surveys designed to measure and compare individual organizations to national benchmarks.
APP: Utilization and Perceptions Survey
Learn more about the APP employment experience within your organization regarding scope of practice, clinical and non-clinical responsibilities, and perceptions on culture and compensation. Specific insights include:
- Organizational structure, support and processes related to the APP workforce
- Roles on the care team specific to location and specialty
- Degree of integration and care team support
- Opportunities for improved utilization and engagement
Physician: APP Utilization and Perceptions Survey
Learn more about your physician workforce and their experience working with APPs. Specific insights include:
- Perception on APP integration and utilization
- Roles of APPs on the care team
- APP impact on quality, access and patient engagement
- Understanding of regulatory requirements
- Opportunities for improved alignment and team performance
These surveys may serve as a resource for organizations looking to better understand the current state of their APP workforce – including quantifying opportunities for optimization and readiness for change – and can play an important part in a more holistic review of APP practices when combined with SullivanCotter’s comprehensive advisory services.
“As health care organizations continue to navigate the lasting effects of a global pandemic, SullivanCotter remains committed to providing them with the critical, data-driven insights they need to measure, analyze and report on compensation and workforce performance. With the goal of addressing the increasingly complex and evolving needs of our clients, we are developing one of the industry’s most comprehensive benchmarking solutions by continuously refining our product roadmap and adding innovative new resources and functionality,” said David Schwietz, Chief Information Officer, SullivanCotter.
To learn more about Benchmarks360™, including important licensing information and a full list of features and functionality, visit sullivancotter.com/benchmarks360 or call 888.739.7039.
About SullivanCotter
SullivanCotter partners with health care and other not-for-profit organizations to understand what drives performance and improve outcomes through the development and implementation of integrated workforce strategies. Using our time-tested methodologies and industry-leading research and information, we provide data-driven insights, expertise, data and technology products to help organizations align business strategy and performance objectives – enabling our clients to deliver on their mission, vision and values.
READ ON NEWSDIRECT

Case Study | Union Health – Population Health Management
Improving Patient Care and Optimizing Financial Performance
DOWNLOAD FULL ARTICLE
As health care continues to shift from productivity and fee-for-service models to more of a quality and performance-based approach, value-based care (VBC) strategies, including population health management (PHM) programs, are becoming a top priority for health care systems across the nation. Leaders within these organizations are searching for more effective and sustainable solutions as they navigate declining reimbursement, regulatory changes, physician burnout and the need for better patient care and lower costs.
These challenges can be addressed with a tailored PHM strategy that supports organizational improvement in the following key areas:
- Maximizing operational processes and outcomes
- Developing a support network for physicians and advanced practice providers (APPs)
- Mitigating risk
- Enhancing performance in a value-based environment
By identifying actionable and targeted opportunities for improvement through a series of evaluations and readiness assessments, Union Health, an integrated, not-for-profit health system based in western Indiana, was able to develop comprehensive VBC and PHM strategies better aligned with their patient-focused approach to coordinated care.
The Situation
As a six-year participant in a local, tertiary accountable care organization (ACO), Union Health had fully outsourced its operational leadership to the parent ACO member. This legacy partnership and arrangement was simply not producing the desired results from a clinical, operational or financial perspective for Union Health – with data and analytics, physician engagement, embedded care management and post-acute care spend being specific areas of concern. Around 2018, Union Health was at a strategic crossroads in regard to its investment in VBC initiatives as the PHM program was not generating the desired results.
This highlighted the need to more effectively integrate operations across departments and service lines, align incentives for leadership and physicians, and reallocate related resources. At the same time, many competing health systems in Indiana were already realizing the benefits of a highly functional PHM program. The leadership at Union Health recognized the key to success would be through a more consistent approach, improved internal processes and engaged leadership.
The organization decided to narrow its focus by strengthening internal capabilities around care management, physician engagement, analytics and reporting to help ensure greater levels of risk-based contracting success with the Centers for Medicare and Medicaid Services (CMS) and other commercial payors.
The Approach
In late 2018, Union Health was presented with an opportunity to partner and align with a nationally recognized health system in a more advanced Next Generation ACO. A Next Generation ACO model offers more risk and reward (both upside and downside risk scenarios) for health systems who already have highly functional internal capabilities in place to support performance. These models represent some of the most advanced value-based arrangements and require greater system-wide operational sophistication. Union Health was looking for a hands-on approach to align initiatives and ensure success.
In order to assess internal operational capabilities, physician and advanced practice provider engagement levels, incentive models and other key functional areas related to VBC, senior leadership at Union Health collaborated closely with SullivanCotter to help quantify this opportunity. After conducting a comprehensive VBC readiness assessment, which included a close examination of the program’s core functional areas such as partnerships, utilization management, attribution and chronic disease management, Union Health elected to partner with the larger health system who had already demonstrated greater success in the Next Generation ACO model. Moreover, Union Health committed to this arrangement for a minimum of two years to support the development of a strong VBC program. Health systems across the country often partner and align with other systems or independent groups to help mitigate risk and better manage overall cost.
SullivanCotter’s primary role with Union Health was to develop and implement an independent PHM program that would help to improve risk-based contracting performance. The program focused on five core principle areas:
- Annual care
- Risk acuity
- Utilization management
- Care management
- Incentive alignment
With these principles in mind and a significant amount of physician and APP input and collaboration, the design of the system’s VBC strategy and approach included the following phases:
To help implement the multi-phased strategy, a task force consisting of Union Health’s executive team and leaders in Business Development, Population Health Management, Physician Services, Utilization Management and Care Management was created to help oversee the process. The initial phase of the project consisted of in-depth interviews with physicians and stakeholders, a thorough review of data and performance metrics, and an operational Readiness Assessment. Key findings from this phase revealed:
- Low engagement from physicians, APPs and other staff with annual care and preventative medicine strategies
- Significant lack of Care Management resources and coordination such as outpatient pharmacy support, discharge planning and risk stratification
- Limited definition of roles and responsibilities for Care Management and Operations team members specific to VBC and PHM
- Insufficient value-based data resources such as reporting capabilities, quality dashboards and clarity surrounding key performance indicators
- Lack of clarity in the scope of practice for nurse practitioners and physician assistants in current team-based care model
- Physician and APP compensation and incentives were not aligned with VBC strategies and initiatives; no incentive for physicians and APPs to enhance value-based performance
- The CMS benchmark or threshold was not met in the contract in order to achieve shared savings – resulting in negative financial impact and poor contract performance
Using the findings from this readiness assessment, SullivanCotter helped executives and physicians at Union Health to further develop a roadmap for the Program Development and Implementation phase.
Roadmap initiatives included the development of:
- Physician and APP educational and engagement materials for workshop sessions
- Clearly defined roles and scope of practice for nurse practitioners and physician assistants in primary care
- Outpatient-focused clinical capacity analysis to support Care Management
- Comprehensive annual care strategy focused on prevention and wellness
- VBC Management team to monitor performance and contract relationships
- Physician and APP incentive components to enhance VBC and PHM
- Standardized dashboards for the entire care team
- Post-acute care strategies more closely aligned with Care Management
- Strategies to monitor ongoing performance
Once the initial components of the roadmap were deployed, the task force worked with SullivanCotter to begin the planning process for two remaining phases within in the PHM model: Physician and APP Incentive Alignment and Performance Review and Monitoring. These processes were also implemented and rolled out during PHM program development and focused on monitoring and enhancing performance in all value-based contracts.
The work accomplished in these two phases included:
- Population health metrics related to annual care, preventative screenings, vaccinations, utilization management, Care Management team engagement and risk-adjustment
- Value-based compensation design concepts and continued education provided to physicians and APPs
- Regular monthly huddles with Care Management team members to review patient volume
- A risk stratification process to determine appropriate care levels for patients
- Physician and APP interviews for feedback and evaluation
- Physician and APP engagement scoring and methodology
- Refinement of key performance indicators
- Development and rollout of physician and APP performance dashboard
The Results
Through the investment in and development of the PHM program and other related VBC initiatives, Union Health was able to achieve the following results over a 12-month period:
- Achieved significant shared savings in year one of the Next Generation ACO as compared to historical performance with improvement of over $6M
- Reduced per member per month spend compared to prior year by 12%
- Implemented a newly redesigned approach to primary care by focusing on team-based care delivery
- Increased the number of completed and billed Medicare Annual Wellness Visits (AWV) from 900 to 5900 with AWV revenue up from approximately $150,000 to $944,000
- Raised the number of documented Care Management team episodes by more than 200%
- Lowered number of emergency room visits in the Next Generation ACO population that were deemed “PCP treatable”
- Documented more than 100 Care Management success stories
- Boosted the clinical diagnosis documentation rate by more than 20%
- Enhanced coordination with post-acute care partners and facilities to help reduce total cost of care for ACO patients by 11%
- Conducted regular meetings and monthly Care Management huddles to enhance physician and APP engagement with knowledge of VBC and PHM concepts and monitoring of individual performance
- Initiated strategic planning to redesign primary care and other specialty compensation models with a focus on performance and value
Tips for Successful VBC/PHM Program Implementation
- Assign dedicated resources to care team optimization
- Collaborate with and gather input from physicians and APPs to strengthen engagement and buy-in
- Align physician and APP incentives to help streamline and reward clinical efforts
- Establish achievable milestones to maintain momentum and engagement
- Conduct regular key stakeholder meetings to provide updates on progress, celebrate successes and course-correct as needed
Lessons Learned
Despite the many factors that differentiate health systems, such as organizational size, complexity, or the communities they serve, there are a common set of fundamental guiding principles and success factors that can be tailored to each organizations’ VBC and PHM strategies.
Union Health’s multi-phase approach – including Readiness Assessment, Program Development and Implementation, Physician and APP Incentive Alignment, and Performance Review and Monitoring – has proven to be an effective way of improving overall performance through the creation of comprehensive VBC and PHM strategies.
Dedicated to enhancing internal capabilities, resources and value-based performance with the objective of improving population health, Union Health partnered with SullivanCotter to develop a long-term, sustainable strategy and implement a comprehensive program to help to improve access and health outcomes for its patients, strengthen physician and APP engagement, and significantly boost financial performance.
Leveraging data-driven insights and over 25 years of experience, SullivanCotter partners with organizations to develop comprehensive value-based care and population health management strategies tailored to the unique needs of each client.
Contact us for more information.

INFOGRAPHIC | Certified Registered Nurse Anesthetists: Compensation and Pay Practices
Detailed insight into CRNA compensation, pay practices, work effort and more
In addition to providing critical base salary and total cash compensation benchmarking information for this important subset of the APP workforce, SullivanCotter’s Advanced Practice Provider Compensation and Productivity Survey has now expanded to include detailed insight into CRNA-specific pay practices as well.
While CRNAs are vital members of this growing workforce, the unique nature of their roles includes key differences in work effort and premium pay practices when compared to other APPs.
View highlights from the 2020 survey results to learn more!
DOWNLOAD INFOGRAPHIC


WEBINAR | The Impact of the Changing Health Care Environment on Primary Care
Is your organization struggling to address the impact of COVID-19, changes to the Stark Law and updates to the Physician Fee Schedule?
Tuesday, April 27 | 10-11am CT
REGISTER TO ATTEND
Hosted by the American Association of Provider Compensation Professionals (AAPCP)
Prior to the onset of COVID-19, the changing reimbursement environment and transition to value-based care were impacting primary care compensation design and pay practices. Today, as health care organizations nationwide are navigating an increasingly complex operating environment, COVID-19 continues to place pressure on financial sustainability, patient access and population health management.
Combined with changes to the Physician Self-Referral Law (Stark) and updates to the 2021 Physician Fee Schedule and Evaluation & Management CPT codes, health care organizations are rapidly engaging in the redesign of their primary care compensation programs.
During this session, SullivanCotter will highlight relevant market trends impacting contemporary primary care compensation design and discuss evolving plan methodologies and approaches as organizations plan for the future.

ON-DEMAND WEBINAR | Optimize Clinical Resources to Support Population Health Management
Understanding the Strategic Impact of a Physician Needs Assessment
Wednesday, May 19 | 12:30-1:30PM CT
VIEW RECORDING
Hosted by the American Hospital Association/Health Forum
Access to market-specific physician supply and demand data is critical as hospitals and health systems look to support growth, enhance value-based care delivery, and reassess cost and efficiency concerns.
Health care organizations must identify the right amount and type of physician specialties to operate effectively in the markets they serve with the goals of optimizing clinical performance as the focus on value-based care and population health management intensifies.
Learn how accurate and actionable data-driven insight can help hospitals and health systems to identify, monitor and respond to changing service needs and physician and advanced practice provider (APP) staffing requirements. Decide strategically whether to recruit, employ or affiliate to create a competitive edge in today’s rapidly evolving health care environment.
During this webinar, industry experts from SullivanCotter will discuss:
- Partnering with Union Health on strategies to support expanded value-based care and population health management requirements
- Evaluating the market-specific drivers that influence physician demand
- Accurately pinpointing employed and affiliated market physicians by specialty
- Leading practices and innovative approaches to inform physician strategy and alignment efforts to enhance performance
- Creating a competitive edge by optimizing clinical resources

Case Study | The Key Role of Advanced Practice Providers in Today's New Normal
Featuring Stanford Health Care's Strategy to Heighten APP Integration and Engagement
As health care organizations nationwide continue to balance managing the immediate implications of the COVID-19 pandemic with planning for what lies ahead, many are looking to optimize team-based care delivery to help address emerging operational challenges, maintain financial sustainability, and meet evolving patient needs.
With the ability to direct patient care and generate revenue, advanced practice providers (APPs) are critical members of the care team and can play an important role in this transformation.
Featuring a case study published in AAPL's Physician Leadership Journal, learn more about how SullivanCotter partnered with Stanford Health Care to develop a comprehensive strategy and program to maximize utilization, support optimization and enhance engagement for its growing APP workforce.
READ FULL ARTICLE

HFMA | Navigating Change: Implications of CMS's 2021 Physician Fee Schedule
Addressing the impact on physician compensation and productivity
Featured in HFMA's hfm Magazine, SullivanCotter discusses changes to the 2021 Physician Fee Schedule and highlights challenges health care organizations and their financial leaders are facing as they look to address the impact on physician and advanced practice provider compensation and productivity.
Due to the magnitude of the changes within the final rule for the 2021 Physician Fee Schedule, organizations with productivity-based physician compensation plans must understand the implications of these changes and on payer payments, productivity levels, survey benchmarks and regulatory compliance.
Learn more about the short- and long-term impact of the changes and different approaches to consider as you move forward with 2021 compensation decisions.
READ FULL ARTICLE
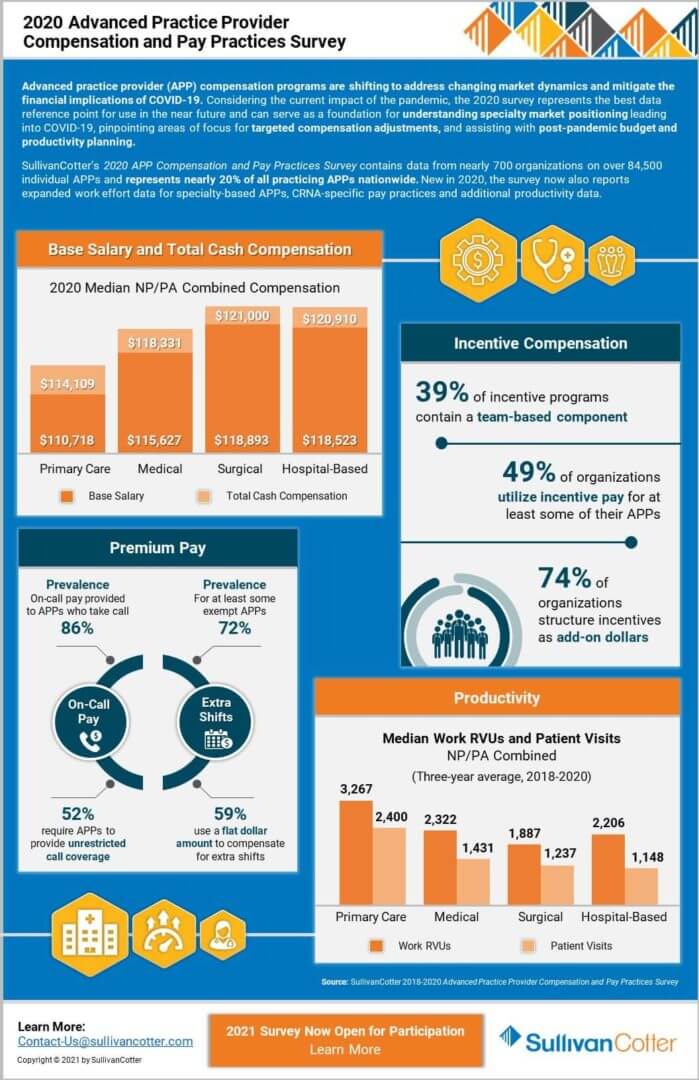
INFOGRAPHIC | 2020 Advanced Practice Provider Compensation and Pay Practices Survey
Representing nearly 20% of all practicing APPs nationwide
Advanced practice provider (APP) compensation programs are shifting to address changing market dynamics and mitigate the financial implications of COVID-19. Considering the current impact of the pandemic, the 2020 survey represents the best data reference point for use in the near future and can serve as a foundation for understanding specialty market positioning leading into COVID-19, pinpointing areas of focus for targeted compensation adjustments, and assisting with post-pandemic budget and productivity planning.
SullivanCotter’s 2020 APP Compensation and Pay Practices Survey contains data from nearly 700 organizations on over 84,500 individual APPs and represents nearly 20% of all practicing APPs nationwide. New in 2020, the survey now also reports expanded work effort data for specialty-based APPs, CRNA-specific pay practices and additional productivity data.
The 2021 survey is now open for participation. Don't miss your chance to submit data and gain access to exclusive APP compensation, pay practices and productivity data!
View highlights from the 2020 results to learn more - including base salary and total cash compensation, incentive compensation, premium pay and clinical productivity.
DOWNLOAD INFOGRAPHIC

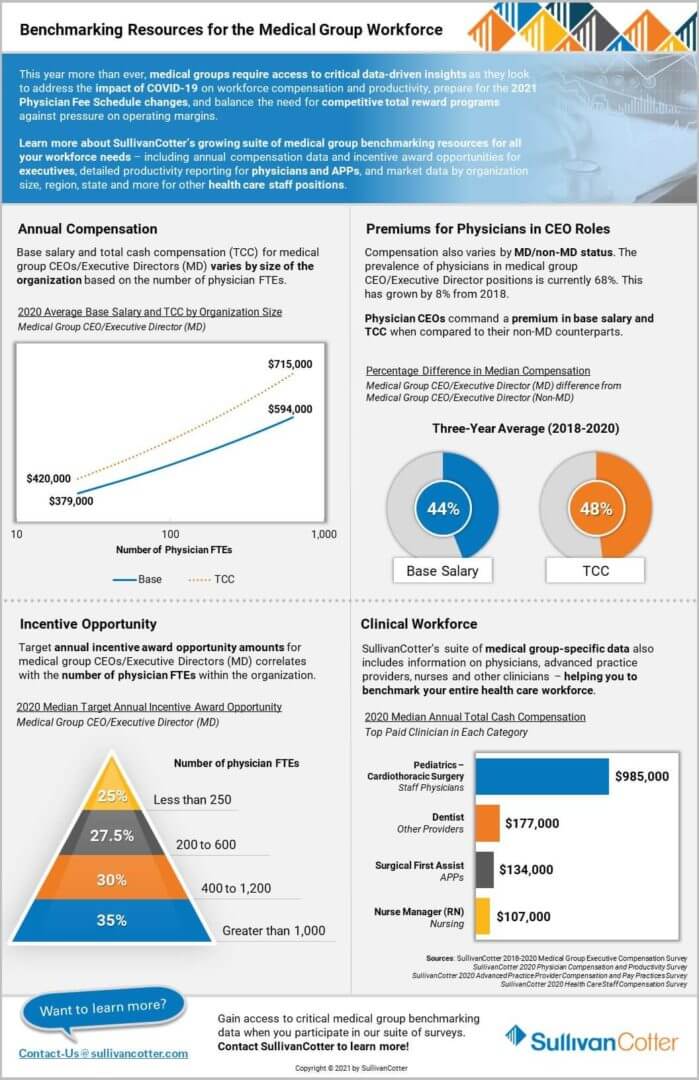
INFOGRAPHIC | Benchmarking Resources for the Medical Group Workforce
Gain access to critical medical group benchmarking data for the entire health care workforce - including executives, physicians, advanced practice providers and other health care staff
This year more than ever, medical groups require access to critical data-driven insights as they look to address the impact of COVID-19 on workforce compensation and productivity, prepare for the 2021 Physician Fee Schedule changes, and balance the need for competitive total reward programs against pressure on operating margins.
Learn more about SullivanCotter’s growing suite of medical group benchmarking resources for all your workforce needs – including annual compensation data and incentive award opportunities for executives, detailed productivity reporting for physicians and advanced practice providers, and market data by organization size, region, state and more for other health care staff positions.
Our suite of 2021 health care compensation surveys are now open for participation!
View highlights from the 2020 results to learn more about SullivanCotter's proprietary benchmarking data and resources available to medical groups.
DOWNLOAD INFOGRAPHIC

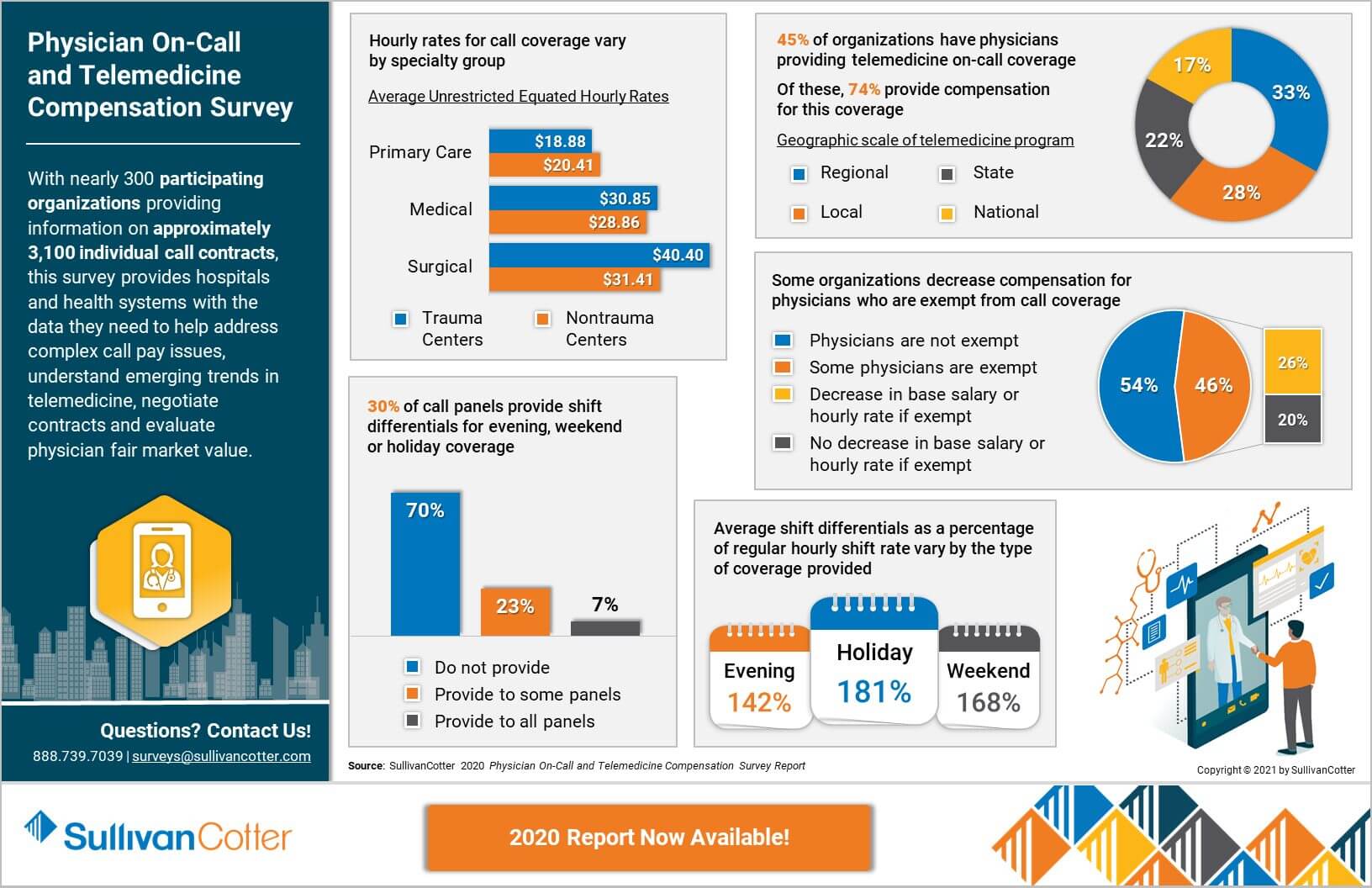
INFOGRAPHIC | 2020 Physician On-Call and Telemedicine Compensation Survey
One-of-a-kind survey providing rare insight into physician call-pay and telemedicine practices
As clinical care settings and practices continue to change in a rapidly evolving health care environment, many organizations are expanding or evaluating their physician on-call and telemedicine programs.
Designing effective arrangements to support this demand is critical, and starts with gaining access to the right data.
With nearly 300 participating organizations providing information on approximately 3,100 individual call contracts, this survey provides hospitals and health systems with the data they need to help address complex call pay issues, understand emerging trends in telemedicine, negotiate contracts and evaluate physician fair market value.
The 2020 survey report is now available for purchase! View highlights from the results to learn more.
DOWNLOAD INFOGRAPHIC

ARTICLE | 10 Best Practices for the Board's Human Capital Committee
Featured in McDermott Will & Emery's new e-book from its Governing Health series
SullivanCotter's Kathy Hastings, Executive Workforce Practice Leader, and Tim Cotter, Managing Director, have contributed to a new e-book from McDermott Will & Emery entitled Key Agenda Items for Board Committees: A Briefing for Governance and Executive Leadership.
Their chapter focuses on the board human capital committee and the key role it plays in guiding human resources strategies as health care organizations face today's challenges. Human capital is critical to organizational strategy, and the committee should test whether the components of the human capital strategy – namely people, process and technology practices – can sustain the organization.

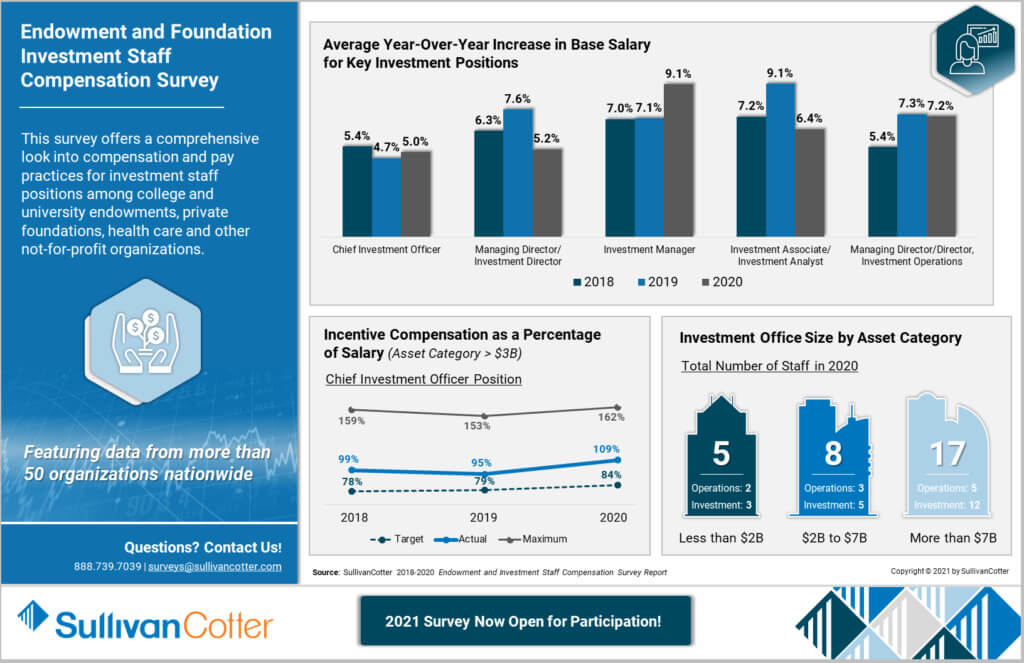
INFOGRAPHIC | 2020 Endowment and Foundation Investment Staff Compensation Survey
Featuring data from more than 50 not-for-profit organizations nationwide
This survey offers a comprehensive look into compensation and pay practices for investment staff positions among college and university endowments, private foundations, health care and other not-for-profit organizations. It also includes detailed insight into the chief investment officer position.
View highlights from the 2020 results, including average year-over-year increase in base salary for key investment positions, incentive compensation as a percentage of salary for the chief investment officer position, and investment office size by asset category.
Don't miss your chance to participate - the 2021 survey is now open! The final deadline to submit is February 26, 2021.
DOWNLOAD INFOGRAPHIC

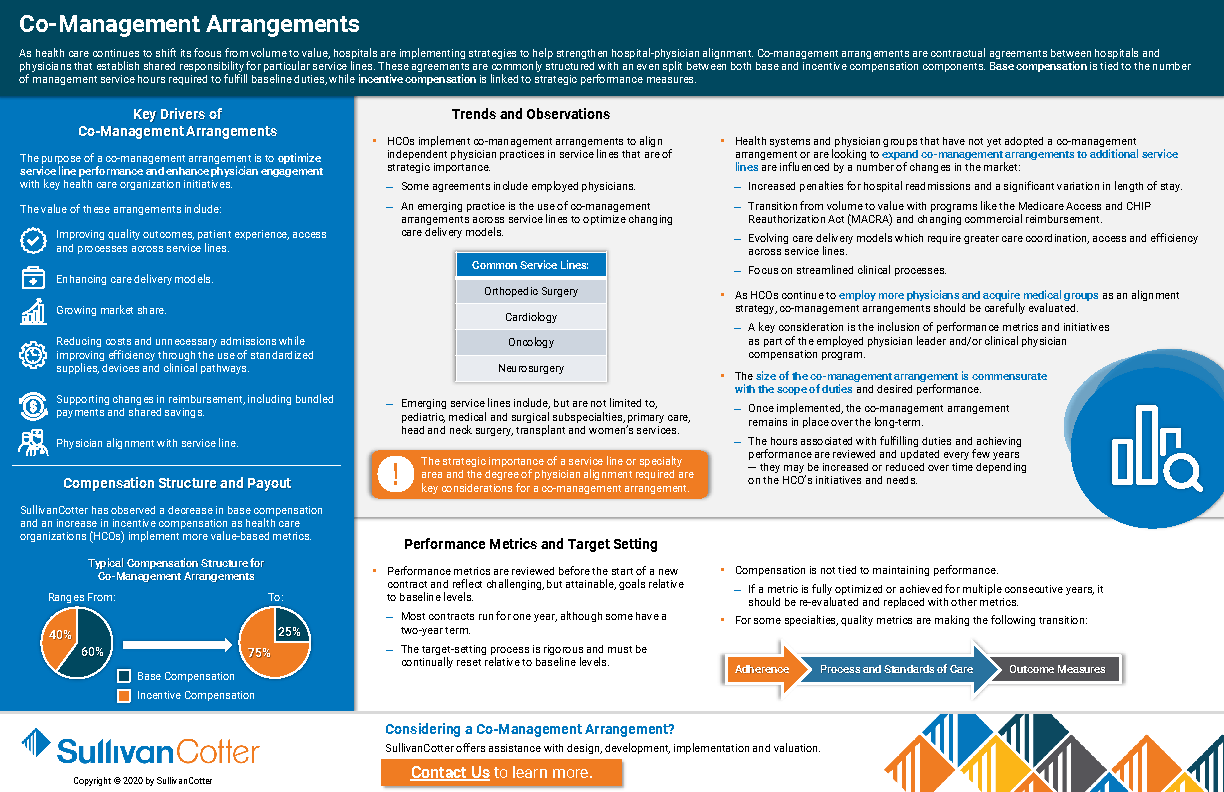
Understanding Co-Management Arrangements
Key drivers, compensation structures and payouts, and performance metrics and target setting
As health care continues to shift its focus from volume to value, hospitals are implementing strategies to help strengthen hospital-physician alignment. Co-management arrangements are contractual agreements between hospitals and physicians that establish shared responsibility for particular service lines. These agreements are commonly structured with an even split between both base and incentive compensation components. Base compensation is tied to the number of management service hours required to fulfill baseline duties, while incentive compensation is linked to strategic performance measures.
DOWNLOAD

PRESS RELEASE | SullivanCotter Integrates Health Care Contract Management Solution into PPMT™
Partnering with Ntracts to deliver full-scale contract lifecycle management capabilities
November 30, 2020 – Chicago – SullivanCotter, the nation’s leading independent consulting firm in the assessment and development of total rewards programs, workforce solutions, and technology and data products for the health care industry and not-for-profit sector, has partnered with Ntracts, a premier health care contract management solution, to incorporate full-scale contract lifecycle management as part of its comprehensive Provider Performance Management Technology™ (PPMT) platform. PPMT™ is an industry-first, cloud-based solution that enables engagement and alignment of the clinical workforce through the automation of performance-based compensation administration, analytical and reporting capabilities. Ntracts allows organizations to mitigate contract compliance risk and streamline the contracting process across the entire enterprise.
Designed to address a spectrum of physician, leadership and other key administrative needs, PPMT™ delivers centralized and actionable data tailored to the unique needs of each stakeholder. It combines years of health care compensation insight and expertise with an intuitive, automated technology platform, and serves as a single source of truth that helps empower physicians to drive desired outcomes and enhance organizational performance.
Ensuring that physician employment agreements align with system-wide compensation terms and payments remains a challenge for health care organizations nationwide. With the addition of Ntracts, PPMT™ will include a cutting-edge contract lifecycle management component that will provide hospitals and health systems with an accurate and comprehensive view of clinical employment contracts across the organization in real-time. By effectively integrating the compensation, performance and contract lifecycle management process into one centralized platform, PPMT™ will help to drive results through greater alignment, transparency and insight.
“Health care continues to evolve at a rapid pace, and there are number of complex moving parts to navigate as it relates to physician compensation and performance. By adding critical contract management capabilities to help health care organizations reduce risk, maintain compliance with changing regulatory requirements, and improve operational efficiency, PPMT™ will be a full-scale solution designed to support the transition from volume to value-based care,” said David Schwietz, Chief Information Officer, SullivanCotter.
David Paschall, Chief Executive Officer of Ntracts, adds, “SullivanCotter shares our commitment to quality and we are proud to combine our industry-leading contract lifecycle management solution with SullivanCotter’s expertise in physician compensation and performance. Together we can offer an unmatched, end-to-end technology solution to support health care organizations as they work to drive change and deliver long-term, sustainable results in this quickly evolving environment.”
For more information on Provider Performance Management Technology™, visit www.sullivancotter.com/PPMT or contact us at 888.739.7039.
About SullivanCotter
SullivanCotter partners with health care and other not-for-profit organizations to understand what drives performance and improve outcomes through the development and implementation of integrated workforce strategies. Using our time-tested methodologies and industry-leading research and information, we provide data-driven insights, expertise, data and technology to help organizations align business strategy and performance objectives – enabling our clients to deliver on their mission, vision and values.
About Ntracts
Ntracts, Inc. offers a software-as-a-service application that enables users to originate, search for and report on contracts. The application also accelerates the contract review and approval process by automatically notifying responsible parties of contract requests, approaching expiration dates and other critical performance milestones, saving clients both time and money. Ntracts, Inc. is based in Indianapolis, Indiana, and was founded by Hall, Render, Killian, Heath & Lyman, the nation's leading health care law firm.
READ ON NEWSDIRECT

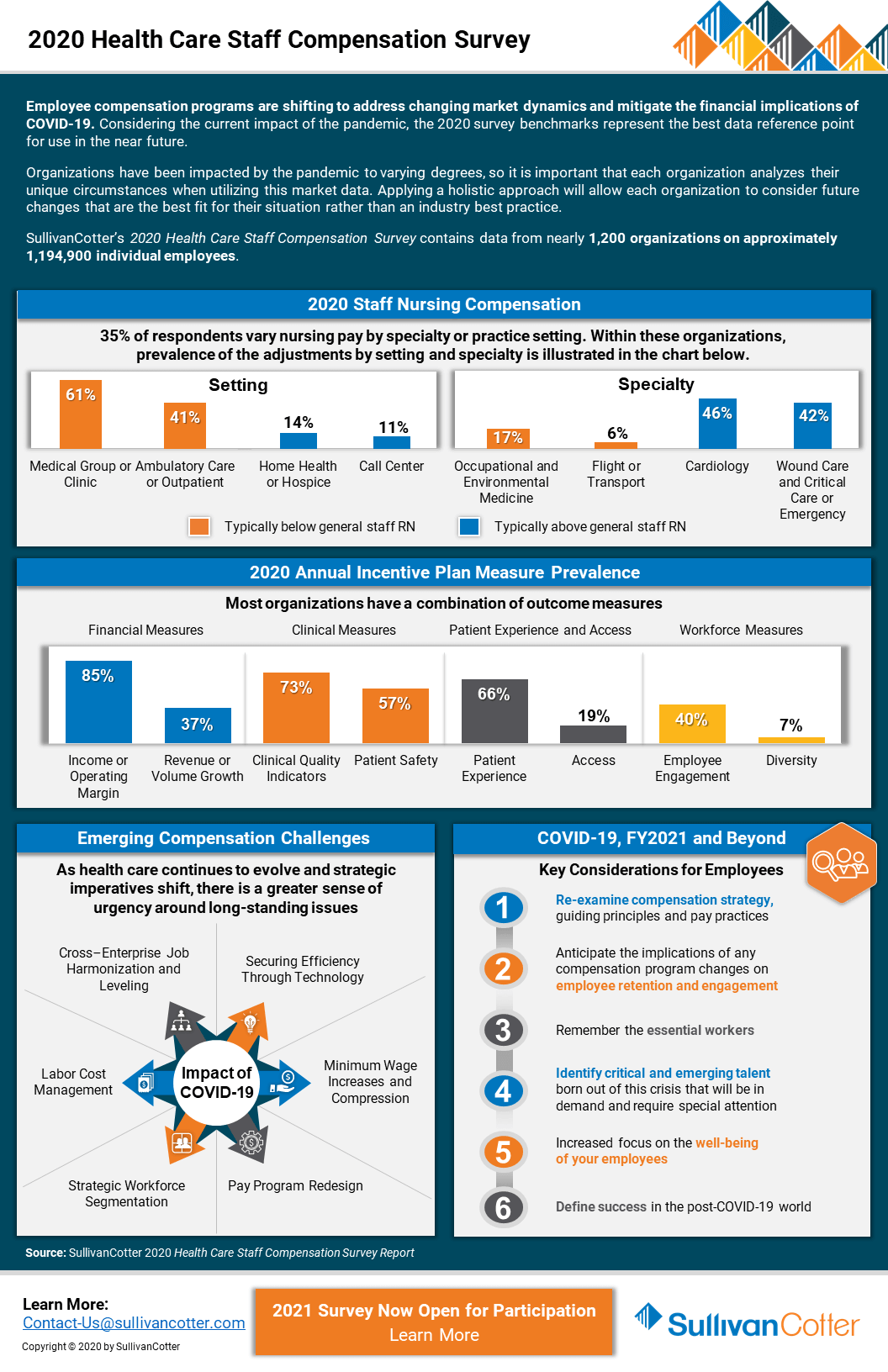
INFOGRAPHIC | 2020 Health Care Staff Compensation Survey
Key considerations for the health care employee workforce during COVID-19 and through 2021 and beyond
Employee compensation programs are shifting to address changing market dynamics and mitigate the financial implications of COVID-19. Considering the current impact of the pandemic, the 2020 survey benchmarks represent the best data reference point for use in the near future.
Organizations have been impacted by the pandemic to varying degrees, so it is important that each organization analyzes their unique circumstances when utilizing this market data. Applying a holistic approach will allow each organization to consider future changes that are the best fit for their situation rather than an industry best practice.
SullivanCotter’s 2020 Health Care Staff Compensation Survey contains data from nearly 1,200 organizations on approximately 1,194,900 individual employees.
The 2021 survey is now open for participation!
DOWNLOAD INFOGRAPHIC

PRESS RELEASE | Annual results from SullivanCotter's Physician Compensation and Productivity Survey
Physician Compensation Programs Shifting to Address Changing Market Dynamics and Mitigate COVID-19 Financial Implications
November 11, 2020 – Chicago – SullivanCotter, the nation’s leading independent consulting firm in the assessment and development of total rewards programs, workforce solutions, and technology and data products for the health care industry and not-for-profit sector, recently released results from the 2020 Physician Compensation and Productivity Survey – which represents data from more than 800 organizations on nearly 244,000 individual physicians and advanced practice providers. The results reflect calendar year 2019 and, as the last set of benchmark data available prior to the onset of COVID-19, this year’s survey will serve as an important resource for organizations needing pre-pandemic compensation reference points for this critical workforce.
“Although the pandemic has created a great deal of uncertainty – with many organizations making near-term modifications to their physician compensation programs as a result – we’re seeing a slow and steady adjustment to the ‘new normal’ as patient volumes have returned to approximately 90% of pre-COVID-19 levels. In some ways, the fallout from COVID-19 has simply accelerated the forces that were driving physician compensation changes prior to the pandemic, and the 2020 survey data will be very important in helping to determine how organizations are responding to these challenges,” said Tim Stamper, Senior Consultant, SullivanCotter.
Physician Total Cash Compensation (TCC)
While TCC has grown, on average, 2.5% annually since 2012, COVID-19-related reductions in surgical and non-emergent care have impacted the financial condition of many health care organizations nationwide – causing them to implement or consider a number of compensation and benefits-related modifications to help offset significant losses in revenue. According to SullivanCotter’s COVID-19 Physician and Advanced Practice Provider Compensation Practices Survey series, nearly 30% of participants had implemented or were considering pay reductions for front line physicians and nearly 40% of participants were doing the same for non-front line physicians as of May 2020. Median pay cuts were 11% and 15% for front line and non-front line physicians respectively. Other organizations made cuts in physician benefits in response to COVID-19. The most common benefit program changes in 2020 included eliminating or reducing retirement plan contributions, adjustments to PTO policies, and eliminating or reducing CME allowances. The majority of these actions were intended to be temporary and, as patient volumes continue to increase and organizations start to recover financially, many are returning to historical pay and benefits practices.
Due to the financial impact of COVID-19, physician incentive programs have also come under scrutiny in 2020. Among respondents surveyed in May, 16% of organizations reported eliminating or reducing non-productivity incentive compensation in 2020 while an additional 38% were considering this action. Many organizations pay out these incentives at year-end, making these programs an obvious target for cost-reduction.
Physician Productivity
The 2020 Physician Compensation and Productivity Survey results continue to show a trend of flat or even declining median work RVU (wRVU) productivity across all major specialty categories. Since TCC showed modest increases in the 2020 survey, TCC per wRVU ratios have also increased. While we have anticipated growth in value-based incentives, wRVUs and productivity-based incentives still determine the majority of incentive or variable compensation as a percentage of TCC. Approximately 70% of organizations utilize wRVUs to determine compensation for primary care and specialist physicians, with wRVU productivity accounting for about 18% of TCC in plans with a base salary component and over 90% of TCC in plans without a base salary component. Less than half (44%) of organizations surveyed include a wRVU component for hospital-based physicians, who are instead paid primarily on base salary and shift-based models.
As organizations focus their attention on maintaining patient access and minimizing the financial losses created by COVID-19, the emphasis on individual wRVU productivity will remain prominent. While the pandemic itself has had a sizable impact on patient volumes and physician productivity, the Centers for Medicare and Medicaid Services’ (CMS) proposed changes to the Evaluation & Management wRVU values loom large as organizations look ahead to 2021. These adjustments include an increase in wRVUs for most office-visit E&M codes due to added responsibilities physicians have absorbed over the last five years. As a result of the overall projected increased in wRVUs, a 10.6% reduction in the conversion factor was required in order to maintain budget neutrality. The proposed increase in wRVU values ranges from 28%-46% for established office visits, which will have a significant impact on compensation plans that use wRVUs as a determinant of compensation.
Considerations for 2020 and Beyond
Although COVID-19 has sharpened industry focus on supporting financial sustainability, other market dynamics and the timing of anticipated financial recovery are also influencing the way hospitals and health systems are approaching physician compensation in both the short and long-term.
“Considering the implications of COVID-19 in 2020 and the impending impact of wRVU changes in 2021, the 2020 survey benchmark data represents the best data reference point for use in the near future. With appropriate context, it can serve as a foundation for understanding specialty market positioning leading into COVID-19, identifying recruitment and retention risks, and pinpointing areas of focus for targeted compensation adjustments as your organization moves forward with 2021 planning,” said Dave Hesselink, Principal, SullivanCotter.
There are a number of important physician compensation considerations for organizations to assess as they continue to navigate the new normal:
- Be mindful of how to appropriately use 2020 survey data. Understand the timing of the data and consider what you are trying to assess before using it. It can be helpful in benchmarking the competitiveness of compensation program elements and incentive opportunities.
- Develop an approach to physician compensation now in response to CMS’ proposed wRVU changes. Organizations should be proactive in assessing how these changes will impact payer reimbursement and physician compensation programs.
- With continued uncertainty regarding the impact of the pandemic in FY2021 and beyond, be prepared for new pandemic-related challenges to patient revenues and physician compensation. Organizations would be well-advised to have a plan developed in advance of any new restrictions on elective and non-emergent care to mitigate additional financial losses.
For more information on SullivanCotter’s surveys or the upcoming Evaluation and Management wRVU value changes, please visit our website at www.sullivancotter.com, email us or contact us by phone at 888.739.7039.
About SullivanCotter
SullivanCotter partners with health care and other not-for-profit organizations to understand what drives performance and improve outcomes through the development and implementation of integrated workforce strategies. Using our time-tested methodologies and industry-leading research and information, we provide data-driven insights, expertise, data and technology products to help organizations align business strategy and performance objectives – enabling our clients to deliver on their mission, vision and values.
READ ON NEWSDIRECT

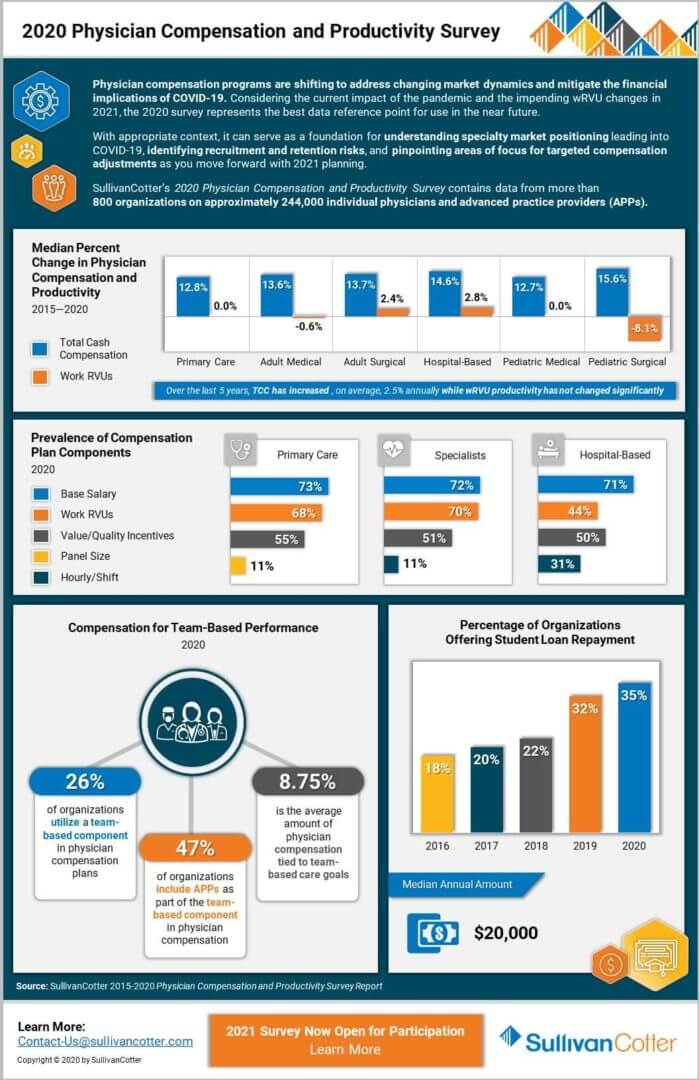
INFOGRAPHIC | 2020 Physician Compensation and Productivity Survey
Utilizing the 2020 survey data to assess the competitiveness of physician compensation programs and incentive opportunities
Physician compensation programs are shifting to address changing market dynamics and mitigate the financial implications of COVID-19. Considering the current impact of the pandemic and the impending wRVU changes in
2021, the 2020 survey represents the best data reference point for use in the near future.
With appropriate context, it can serve as a foundation for understanding specialty market positioning leading into COVID-19, identifying recruitment and retention risks, and pinpointing areas of focus for targeted compensation adjustments as you move forward with 2021 planning.
Learn more from SullivanCotter’s 2020 Physician Compensation and Productivity Survey - which contains data from more than 800 organizations on approximately 244,000 individual physicians and advanced practice providers (APPs).
The 2021 survey is now open for participation!