The Perils of Payment
Effectively addressing the challenges associated with physician compensation and financial arrangements is a key component for governing boards striving to meet strategic objectives in a high-risk and complex health care environment.
In the July/August 2014 issue of Trustee magazine, Kim Mobley, Managing Principal and National Physician Compensation Practice Leader, and Marc Hallee, Consulting Principal, address compensation issues. The article, titled “The Perils of Payment,” outlines the varying types of physician and financial arrangements that are emerging. It provides a checklist of activities to support effective risk management and board oversight of physician compensation and questions to consider when formulating your organization’s approach to this intricate issue.
Executive Summary of the 2014 Employee Benefits Practices in Hospitals and Health Systems Survey
In its third annual survey of hospital and health system employee benefits practices, SullivanCotter compiled and analyzed information from many of the top hospitals and health systems across the country to help answer the questions listed above. Unlike research that includes insurance companies, pharmaceutical manufacturers and other organizations related to the health care sector, this survey focuses solely on hospitals and health systems.
Download the Executive Summary
Principal Dave Hesselink Addresses The Healthcare Roundtable
For more information on this meeting, please visit The Healthcare Roundtable website by clicking here.
Andrew Lewis Slated Addresses the Nebraska Hospital Association’s Annual Convention
SullivanCotter Principal Andrew Lewis addressed the attendees of the 2014 Nebraska Hospital Association Annual Convention. This year's event was held October 22-24 in Lincoln, Nebraska at The Cornhusker Marriott Hotel.
The NHA Annual Convention is the largest gathering of health care professionals in the state and brings together hundreds of health care professionals to gain insight on leadership, new technology and industry trends, quality excellence and human motivation.
For more information, click here.
Consulting Principal Deb Slater Addresses the IAHA 2014 Annual Health Law Symposium
The Illinois Association of Healthcare Attorneys selected Deb Slater to speak at the 32nd Annual Health Law Symposium which washeld in Chicago.
For more than 30 years, the IAHA Annual Health Law Symposium offers Illinois health care attorneys a day long educational program featuring presentations by nationally recognized experts. The symposium also offered an annual health law primer for lawyers new to the field or veterans wishing to catch up on recent developments.
For more information, click here.
Physician On-Call Pay: Compliance Considerations and Emerging Trends
Physician On-call Pay: Compliance considerations and emerging trends
On-call pay is a hospital’s payment for access to physicians who provide call coverage. Over the past several years, the provision of on-call pay has continued to increase. Therefore, it is important from a strategic, financial and regulatory perspective to properly structure physician on-call pay arrangements.
When structuring on-call pay arrangements, organizations are cautioned to consider regulatory issues, including the Stark Law and Anti-Kickback Statute. Each of these requires that physician compensation arrangements, including on-call pay arrangements, fall within fair market value and are commercially reasonable. Penalties for noncompliance are severe and can include fines of $11,000 per claim as well as treble damages for false claims. Exclusion from Medicare and Medicaid programs, intermediate sanctions and imprisonment may also result.
The Department of Health and Human Services Office of Inspector General (OIG) has issued three helpful advisory opinions concerning physician on-call pay arrangements (07-10, 09-05, 12-15). Each addresses specific factors for consideration:
- Physicians are paid for “tangible” services as opposed to lost opportunity.
- Compensation for call coverage is calculated in advance of services being provided.
- Only select physician groups and physicians within a particular specialty are not offered on-call pay (i.e., call pay
should be offered to all physicians providing services within a particular specialty area). - Aggregate on-call payments are proportionate to physicians’ regular practice income.
- Physicians are responsible for providing, without additional compensation, both inpatient and follow-up care to patients
they admit.
The majority of organizations provide call pay to individual physicians. There are other methods, however, for determining the distribution of the call pay funds. SullivanCotter’s 2013 Physician On-Call Pay Survey summarizes these distribution methods.

Due to declining reimbursement and increasing physician demands, hospitals are often challenged to meet their emergency department (ED) and trauma call panel requirements. As such, the prevalence and associated expenditures of physician on-call pay continue to rise, a trend illustrated by the survey results in the chart below.

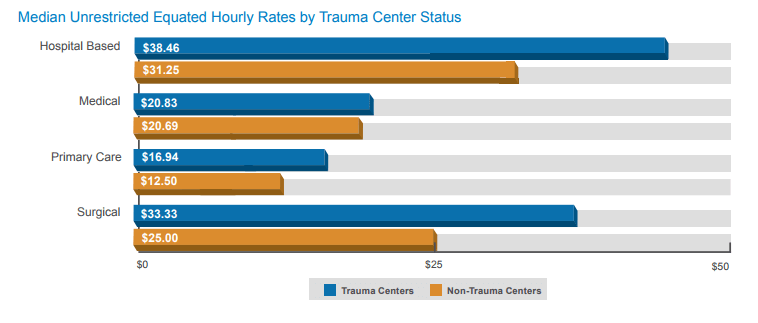
Survey participants indicated that three-quarters of physicians providing on-call coverage receive some form of on-call pay. Payment is typically provided in the form of a stipend or an hourly rate. Some examples of median equated hourly rates for unrestricted call coverage are shown in the table below.

In addition to physician specialty area, several factors, including an organization’s trauma center status, may affect the on-call pay amount. The graph below shows the median equated hourly rates for unrestricted call coverage at trauma and non-trauma centers by combined specialty categories.
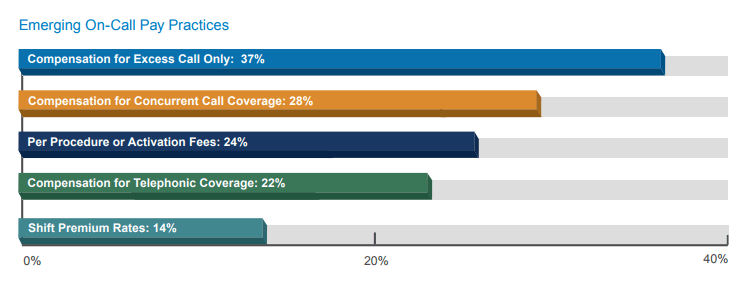
There are a number of different and evolving types of on-call pay arrangements. Key emerging pay practices related to the provision of call pay and their prevalence, as reported by survey participants, are shown in the graph below.
Compensation plan checklist for on-call pay arrangements
Consider the following factors when developing or reviewing an on-call pay arrangement:
- Physician Specialty Area: On-call pay rates vary significantly by specialty area. Surgical specialties are
generally paid more than medical specialties. - Frequency of Call Coverage: The amount of call coverage physicians provide is an important factor when
evaluating whether on-call pay is appropriate and reasonable and can affect the actual rate paid for coverage. - Number of Available Physicians on the Call Panel: The fewer the physicians who are available to serve on
a call panel, the more shifts of call coverage each physician on the panel must provide. This added burden
increases the likelihood that the physicians will receive on-call pay. - Likelihood of the Physician to Be Called In: Specialties in which physicians are most likely to be called in tend
to receive the highest on-call pay rates. - Acuity of Care: Physicians serving on a trauma call panel are more likely to be compensated for call coverage,
and their rates are generally higher than those of physicians providing general ED coverage. - Provisions for Uncompensated Care: Consideration should be given to the patient population. In environments
with large uninsured or under insured populations, the likelihood increases that physicians will require call pay. - Employed Physician Call Pay: Call pay for employed physicians should not overlap with any base salary they
receive for clinical work during the call coverage period.
Key Terms
- Commercial Reasonableness: The broader business issues associated with a compensation arrangement (e.g., a
demonstrated community need for a particular specialty or service). - Concurrent Call Coverage: Arrangement in which a physician provides on-call coverage for more than one hospital
within the system during the same period of time. - Excess Call: Compensation for call coverage paid only after a specified amount of uncompensated coverage has
been provided. - Fair Market Value: The value in arm’s-length transactions, consistent with the general market value (i.e.,
compensation that would be included in a service agreement as the result of bona fide bargaining between wellinformed
parties not otherwise in a position to generate business for one another at the time of the agreement). - General ED Call: Call coverage provided for general ED services.
- Restricted Call: Physician must remain on the premises for duration of call coverage shift.
- Telephonic Call: Compensation to treating physicians for providing telephonic consultations with no immediate
obligation to present to the hospital. - Trauma Call Coverage: Call coverage provided for trauma services only.
- Unrestricted Call: Physician is not required to remain on the premises but must respond to calls within a specified
time frame.
As health care reimbursement shifts from volume- to value-based patient-focused care, new models of compensation are emerging for physicians and advanced practice clinicians. SullivanCotter specializes in working with health care organizations to align physician recruitment, retention and productivity strategies with quality outcomes, patient satisfaction and efficiency through effective compensation approaches. We know the physician labor market as well as compensation and benefits trends and we understand the need to compete for medical talent.
In its ninth year, SullivanCotter’s 2013 Physician On-Call Pay Survey delivers comprehensive benchmarking data detailing on-call pay rates for more than 130 organizations and more than 40 physician and advanced practice clinician specialties, including more than 1,300 individual call panels. This annual survey is the only one of its kind that reports rates by physician specialty and type of on-call pay.
Jim Rohan and Jason Tackett Present “Aligning Physician Compensation – The Journey from Volume to Value”
Vice President and Managing Director Jim Rohan and Principal Jason Tackett addressed the July 16th meeting of the Metropolitan Chicago Healthcare Council. This half-day interactive program for executive, managers and specialists involved in physician compensation will cover the following topics:
- The new era - payment reform driving care delivery transformation
- Other key trends impacting physician compensation design
- Physician alignment - post acquisition of private practices and the development of an integrated medical group
- Aligning physician compensation (for employed physicians) with enterprise strategies and incentives
- Physician compensation plans - current state and future state
- Physician incentive compensation design
- Productivity incentives, quality incentives, service incentives, etc.
- Individual vs. group goals/metrics (access, panel size, quality, patient satisfaction, efficiency, etc.)
- Plan design from a change management perspective
- Regulatory considerations
- Open forum - participants' share their experiences (what works and what doesn't)
For more information, please click here.
Tom Pavlik and Aria Glasgow Address Metropolitan Chicago Healthcare Council
Speaking on the topic "“Pay for Performance in Health Care Provider Organizations,” this half-day program introduced members of the MCHC to concepts and practices related to pay-for-performance. This skill-building program focused on contemporary compensation design approaches, using real world examples and health care specific market practices.
For more information, click here.
SullivanCotter’s Craig Pederson Speaks at HFMA's 2014 Annual National Institute
The Healthcare Financial Management Association's 2014 Annual National Institute included SullivanCotter Principal Craig Pederson among its list of speakers. Along with co-presenter Kurt Ebbers of the Hannibal Clinic, Craig discussed "Multispecialty Group Perspective on Physician-Hospital Alignment." Their presentation examined the complete physician-hospital alignment journey from beginning to end through the eyes of an independent physician group.
For more information on this event, please click here.
SullivanCotter Data Reflected in "Shift in Payment Models Alters Physician Compensation"
HealthLeaders Media relied on SullivanCotter's 2013 Physician Compensation and Productivity Survey data to examine the benchmarks affecting physician reimbursement levels in the April 3, 2014 article. Insight from Managing Principal and National Physician Compensation Practice Leader Kim Mobley are also included.
Pay Gap Between Specialists, Primary Care Physicians Diminishing, According to Becker's Hospital Review Article
Referencing data from the SullivanCotter Physician Compensation and Productivity Survey, Becker's Hospital Review examines trends in physician compensation levels in their February 26, 2014 article.
SullivanCotter Names John Collins as Principal in Executive Compensation and Welcomes Back Marc Hallee as Consulting Principal
CHICAGO – SullivanCotter, one of the nation’s leading independent compensation, benefits and human resources management consulting firms, has named John Collins as a Principal in its Executive Compensation practice and announced that Marc Hallee has rejoined the firm as a Consulting Principal in its Physician Compensation practice.
John Collins – Principal, Executive Compensation
Mr. Collins joins SullivanCotter with over 20 years of experience in compensation and benefits consulting for a variety of for-profit and not-for-profit organizations. His experience encompasses design and implementation of annual and long-term incentive plans, nonqualified deferred compensation sales incentive plans and benefits strategy design. Prior to joining SullivanCotter, Mr. Collins worked at Towers Watson, where he was a Principal and the Director of Executive Compensation and Rewards in New York. He has a Bachelor of Arts in mathematics from The State University of New York in New York and a Master of Business Administration with a concentration in finance from Columbia Business School in New York.
“We would like to welcome John to the SullivanCotter team,” said Chris Terranova Asselta, Managing Director of SullivanCotter’s Eastern region. “John’s extensive background in executive compensation and benefits consulting will help elevate SullivanCotter’s capabilities to better serve our clients in the for-profit and not-for-profit sectors.”
Marc Hallee – Principal, Physician Compensation
Mr. Hallee returns to SullivanCotter with more than 20 years of experience in compensation and benefits program redesign and overseeing compensation strategies and programs for physicians. He formerly served as Executive Vice President and Chief Human Resources Officer at Scott & White Healthcare in Texas, where he oversaw the strategy and programming for a $2.2 billion health system for more than 14,000 employees. Mr. Hallee has a Bachelor of Arts in economics from Bates College in Maine and a Master of Business Administration in leadership and change management from DePaul University in Illinois.
“As health systems continue to change and evolve, Marc truly understands the real life issues associated with managing physician relationships,” said Jim Rohan, Managing Director of SullivanCotter’s Central region. “His experience as the Chief Human Resources Officer of a major health system in Texas will also be valuable as SullivanCotter continues to look at ways to better meet our clients’ needs in that region.”
SullivanCotter’s 2013 Manager and Executive Compensation Survey Highlights Variation in Salary Increases Among Emerging Positions
SullivanCotter, a human resources and total compensation consulting firm, released the results of its 2013 Manager and Executive Compensation in Hospitals and Health Systems Survey. According to research findings, 2013-budgeted and 2014-projected salary increases for executives have continued at 3%, with greater variation being seen in emerging health care industry positions. Jobs experiencing the highest increases annually include the medical informatics executive (6.5%), the business development executive (11.6%), the ambulatory care executive (8.5%) and the quality management executive (8.4%).
“Due to the mergers and acquisitions in health care and continued reimbursement and cost-cutting concerns, we are seeing changing roles and scopes of responsibility for executive positions, which will affect how executives are paid by both the level and the manner of pay,” said SullivanCotter Executive Compensation Practice Leader Kathy Hastings. “While the general trend is to budget the same level for executive increases as for non-executive employees, organizations are making market adjustments as needed to address the changing scope of responsibilities and recruitment and retention concerns.”
The SullivanCotter Manager and Executive Compensation in Hospitals and Health Systems Survey is the largest survey of its kind for hospitals and health systems nationwide. It provides data to help health care industry leaders meet the challenges of regulatory compliance and performance-driven executive compensation.
“The 2013 survey also provided us with data on new jobs representing emerging roles in the marketplace, such as chief patient experience officer, top accountable care executive and top clinical integration executive,” added Managing Principal Tom Pavlik.
Last year’s report contained data from over 1,300 responding organizations comprising more than 300 health systems and 1,000 hospitals, including data for nearly 23,000 executives and managers. The 2014 survey includes new simplified reporting, particularly around organizational characteristics and background information on the organization. In addition, 35 new positions were added, such as head of accountable care organization (ACO) physician network development, health plan top information services executive, head of innovation and ACO chief medical officer, among others.
Now in its 22nd year, the 2014 survey is open for participation through the SullivanCotter Client Portal. For more information on SullivanCotter surveys, registration or participation, please visit our website or contact us by phone at 888.739.7039.
Addressing APC and Staff Pay Disparities
The SullivanCotter white paper titled “Staff and Advanced Practice Clinician Compensation Programs: Addressing Payroll Disparities to Improve Value and Reduce Cost” outlines an approach to help health care organizations understand market standards and best practices to effectively manage APC and staff compensation. Gain additional insight from the paper's case studies that review how two prominent health care systems approached their special pay compensation challenges.
SullivanCotter’s Physician Compensation Survey Reveals Decreasing Gap Between Primary Care and Specialty Physician Compensation
SullivanCotter (SullivanCotter), a health care compensation and human resources management consulting firm, reported that data for physician total cash compensation levels indicate a slight decrease in the gap between primary care physicians and specialists, according to the 2013 Physician Compensation and Productivity Survey Report.
The survey results indicated an overall increase of median total cash compensation of 5.7% for primary care physicians between 2012 and 2013. Conversely, medical and surgical specialists had an increase of 3.2% and 2.3%, respectively, during the same time frame.
“For many years, our survey results have shown a widening gap in the pay relationships between primary care physicians and specialists. The results from our 2013 survey demonstrate a slight shift in the market and these pay relationships. This is consistent with the ever-increasing labor market demand for primary care physicians. With the expanded health care coverage and emphasis on preventative care, population health management and cost control, primary care physicians are in high demand as they are at the forefront of ensuring successful implementation of these initiatives,” notes Kim Mobley, Managing Principal and National Physician Compensation Practice Leader.
Other Key Findings
The survey also found health care organizations are modifying their physician compensation plans. While clinical productivity, utilized by about two-thirds of organizations and most often based on work relative value units (work RVUs) continues to be part of the physician compensation model, many organizations are developing transitional approaches that allow them to include other performance-based metrics such as quality, patient satisfaction and, in some instances, citizenship. The prevalence and amount of compensation tied to these metrics have grown significantly over the past few years, with about one-third reporting the use of quality metrics in their physician compensation plan in 2013. Ms. Mobley indicates that “the amount of compensation paid for achievement of specified quality metrics varies by specialty area.” According to the survey, the overall median amount paid for quality in 2013 was $15,000; however, this varied from $7,000 median quality payments for primary care to $20,000 for medical and surgical specialties. When considered as a percentage of total cash compensation, the overall median amount paid for quality was 5.0%. Ms. Mobley further notes that “we are closely monitoring the amount of compensation tied to quality and patient satisfaction as this will have an impact on future compensation approaches. As reimbursement shifts from fee for service to value based, we expect to see some shifts in the balance of the compensation elements that comprise physician compensation plans.”
Other physician compensation trends published include the continued use of on-call pay, as 64% of health care organizations reported paying at least some physicians for call coverage (up from 48% in 2008); the use of non-compete agreements, as reported by two-thirds of the survey participants; and the use of hiring bonuses, as reported by 74% of the survey participants. It should also be noted that physician benefits are an important part of the total compensation provided to physicians. The 2013 survey found that 44% of physician employers provided benefits to physicians that were more generous than those provided to other employees, which is up from 37% in 2012.
The survey report contains data from 484 organizations covering over 91,000 health care providers. It includes total cash compensation data on 230 physician, PhD and advanced practice clinician (APC) specialties, as well as eight medical group executive positions. The full survey report is now available for purchase.
SullivanCotter also announced the launch of its 2014 Physician Compensation and Productivity Survey, which includes improvements to the Client Portal for faster, easier participation, especially for past participants who are now able to pre-populate questions with responses from their 2013 survey submission.
For more information on the 2013 survey results, or to participate in the 2014 survey, please contact the SullivanCotter Survey Team at 888.739.7039 or surveys@sullivancotter.com.
Agenda for Executive Compensation Committee: Minimizing Regulatory and Reputational Risk by Managing Director Timothy Cotter Published
The American Hospital Association's Center for Healthcare Governance published an article by Managing Director Timothy Cotter in its Winter 2013 edition of its Great Boards newsletter. In "Agenda for Executive Compensation Committee: A Guide for Minimizing Regulatory and Reputational Risk," Tim examines the challenges facing executive compensation committees in meeting the demand for executives with proven leadership abilities alongside increased scrutiny from regulators.
For more information on the American Hospital Association's Great Boards, please visit their website.
Survey Reveals Advanced Practice Clinician Workforce Continues to Grow and Incentive Pay Is an Increasing Part of the Compensation Mix
February 12 – CHICAGO – Findings released in the 2013 Advanced Practice Clinician Compensation and Pay Practices Survey Report highlight the continuing high demand for advanced practice clinicians (APCs). The report details survey research conducted by the American Medical Group Association (AMGA), a trade association representing medical groups and integrated health systems and SullivanCotter (SullivanCotter), a health care compensation and human resources management consulting firm. The survey revealed that approximately 2/3 of organizations reported an increase in their APC workforce within the past 12 months and 2/3 projected an increase within the next 12 months.
With the continued growth of the APC profession, there has also been an increase in the number of organizations that have APCs serving in administrative roles. This year, 31% of responding organizations indicated that some of their APCs serve in administrative roles, which is an increase from 20% in 2012. In addition, 14% of responding organizations indicated that APCs report to a director of APCs in 2013, compared to 1% in 2012. “This increase may signal a move toward integrating APCs across systems and developing a more comprehensive strategy for managing this important provider group,” Kay Jensen, Principal and Employee Compensation Practice Leader for SullivanCotter, stated.
Total cash compensation varied by broad specialty area, ranging from nurse practitioners and physician assistants in medical specialties earning a median of $97,858 and $97,272, respectively, to a median of $104,000 earned by both nurse practitioners and physician assistants in hospital-based specialties.
While base or guaranteed salary continues to be the primary component of cash compensation for APCs, 45% of respondents use a combination of base or guaranteed salary and incentive pay for at least some of their APCs. In particular, the top measures used by participants for nurse practitioners and physician assistants are work RVUs and quality. When these incentives are provided, they contribute a median of approximately 10% of all compensation plan components.
"These findings provide hard data to demonstrate the importance of APCs in the future of health care delivery," said AMGA President and Chief Executive Officer Donald W. Fisher, Ph.D., CAE. "For years, we have seen the movement towards a more team-based, coordinated approach to patient care. As more and more groups expand these models throughout their organizations, this survey provides a tool to systematically track and benchmark changes in this area, which will help them in their strategic and financial planning for continued growth and success."
Over 300 health systems, hospitals and physician group practices participated in the survey. Total cash compensation data were submitted for more than 27,000 certified registered nurse anesthetists, nurse midwives, nurse practitioners and physician assistants across 83 specialties. Data are effective July 1, 2013. The survey not only provides total cash compensation data for APCs, but also data on pay practices such as on-call pay, shift differentials, compensation plan components and supplemental benefits.
The 2013 Advanced Practice Clinician Compensation and Pay Practices Survey Report is now available for purchase. If you have any questions about the report, please visit www.sullivancotter.com or email surveys@sullivancotter.com.
About American Medical Group Association
The American Medical Group Association (AMGA) represents medical groups and organized systems of care, including some of the nation’s largest, most prestigious integrated health care delivery systems. More than 150,000 physicians practice in AMGA member organizations, providing health care services for 120 million patients (nearly one in three Americans). Headquartered in Alexandria, Virginia, AMGA is the strategic partner for these organizations, providing a comprehensive package of benefits, including political advocacy, educational and networking programs, publications, benchmarking data services and financial and operations assistance. For more information, visit www.amga.org or call 703.838.0033.
About SullivanCotter
SullivanCotter is the leading independent consulting firm in the assessment and development of tailored total compensation and reward programs for the health care industry. For more than 20 years, the Firm has provided executive, physician and employee compensation and governance counsel to a wide variety of health care and higher education organizations, public charities, associations and foundations. A recognized leader in compensation benchmarking trends and analyses, SullivanCotter has also developed the most widely recognized physician and health care executive compensation surveys in the United States. Building from this unparalleled data, the Firm works closely with executives, boards and compensation committees to devise innovative solutions to attract and retain talent while satisfying business objectives and regulatory requirements. For more information, visit www.sullivancotter.com or call 888.739.7039.
Executive Compensation for Tax-Exempt Organizations
The IRS recently released the Final Report of its Colleges and Universities Compliance Project, in which they examine practices regarding executive compensation and other business activities of tax-exempt colleges and universities. Although the report pertains to higher education institutions, its findings have broader implications for the executive compensation governance practices of all tax-exempt organizations. To help organizations ensure that their executive compensation governance processes are above reproach, SullivanCotter has summarized the key findings and takeaways relevant to executive compensation.
Read the full Compensation Insight
"Ten Most Important Matters Your CEO Should Know About His or Her Employment Contract"
SullivanCotter Managing Director Kathy Hastings co-authored an examination of CEO contract considerations along with Ralph E. DeJong of McDermitt Will & Emery LLP, published in the Winter 2014 edition of Practical Tax Lawyer.
David Cohn Tapped as Speaker at AHLA's In-House Counsel Program and Annual Meeting
The American Healthcare Lawyer's Association tapped David Cohn as a speaker at its 2013 In-House Counsel Program and Annual Meeting, held June 30-July 3, in San Diego.
Along with co-presenter Mary Samsa of MWE, Cohn discussed the "Top Five Challenges for In-House Counsel on Executive Pay."
For more information on this event, please click here.