Physician On-Call Pay: Compliance Considerations and Emerging Trends
Physician On-call Pay: Compliance considerations and emerging trends
On-call pay is a hospital’s payment for access to physicians who provide call coverage. Over the past several years, the provision of on-call pay has continued to increase. Therefore, it is important from a strategic, financial and regulatory perspective to properly structure physician on-call pay arrangements.
When structuring on-call pay arrangements, organizations are cautioned to consider regulatory issues, including the Stark Law and Anti-Kickback Statute. Each of these requires that physician compensation arrangements, including on-call pay arrangements, fall within fair market value and are commercially reasonable. Penalties for noncompliance are severe and can include fines of $11,000 per claim as well as treble damages for false claims. Exclusion from Medicare and Medicaid programs, intermediate sanctions and imprisonment may also result.
The Department of Health and Human Services Office of Inspector General (OIG) has issued three helpful advisory opinions concerning physician on-call pay arrangements (07-10, 09-05, 12-15). Each addresses specific factors for consideration:
- Physicians are paid for “tangible” services as opposed to lost opportunity.
- Compensation for call coverage is calculated in advance of services being provided.
- Only select physician groups and physicians within a particular specialty are not offered on-call pay (i.e., call pay
should be offered to all physicians providing services within a particular specialty area). - Aggregate on-call payments are proportionate to physicians’ regular practice income.
- Physicians are responsible for providing, without additional compensation, both inpatient and follow-up care to patients
they admit.
The majority of organizations provide call pay to individual physicians. There are other methods, however, for determining the distribution of the call pay funds. SullivanCotter’s 2013 Physician On-Call Pay Survey summarizes these distribution methods.
Due to declining reimbursement and increasing physician demands, hospitals are often challenged to meet their emergency department (ED) and trauma call panel requirements. As such, the prevalence and associated expenditures of physician on-call pay continue to rise, a trend illustrated by the survey results in the chart below.
Survey participants indicated that three-quarters of physicians providing on-call coverage receive some form of on-call pay. Payment is typically provided in the form of a stipend or an hourly rate. Some examples of median equated hourly rates for unrestricted call coverage are shown in the table below.
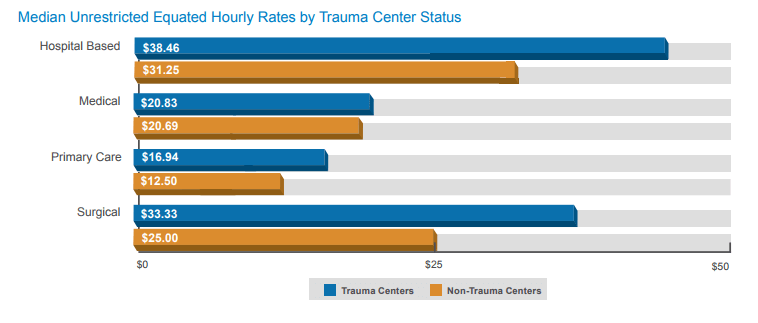
In addition to physician specialty area, several factors, including an organization’s trauma center status, may affect the on-call pay amount. The graph below shows the median equated hourly rates for unrestricted call coverage at trauma and non-trauma centers by combined specialty categories.
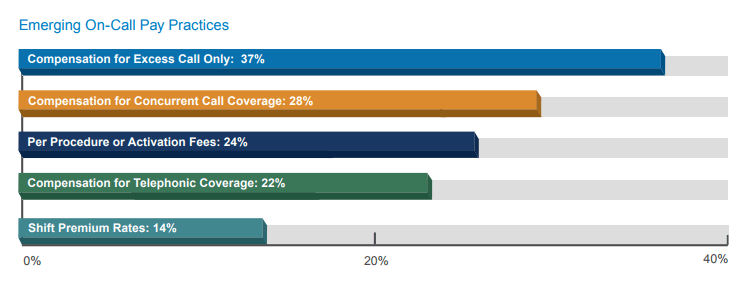
There are a number of different and evolving types of on-call pay arrangements. Key emerging pay practices related to the provision of call pay and their prevalence, as reported by survey participants, are shown in the graph below.
Compensation plan checklist for on-call pay arrangements
Consider the following factors when developing or reviewing an on-call pay arrangement:
- Physician Specialty Area: On-call pay rates vary significantly by specialty area. Surgical specialties are
generally paid more than medical specialties. - Frequency of Call Coverage: The amount of call coverage physicians provide is an important factor when
evaluating whether on-call pay is appropriate and reasonable and can affect the actual rate paid for coverage. - Number of Available Physicians on the Call Panel: The fewer the physicians who are available to serve on
a call panel, the more shifts of call coverage each physician on the panel must provide. This added burden
increases the likelihood that the physicians will receive on-call pay. - Likelihood of the Physician to Be Called In: Specialties in which physicians are most likely to be called in tend
to receive the highest on-call pay rates. - Acuity of Care: Physicians serving on a trauma call panel are more likely to be compensated for call coverage,
and their rates are generally higher than those of physicians providing general ED coverage. - Provisions for Uncompensated Care: Consideration should be given to the patient population. In environments
with large uninsured or under insured populations, the likelihood increases that physicians will require call pay. - Employed Physician Call Pay: Call pay for employed physicians should not overlap with any base salary they
receive for clinical work during the call coverage period.
Key Terms
- Commercial Reasonableness: The broader business issues associated with a compensation arrangement (e.g., a
demonstrated community need for a particular specialty or service). - Concurrent Call Coverage: Arrangement in which a physician provides on-call coverage for more than one hospital
within the system during the same period of time. - Excess Call: Compensation for call coverage paid only after a specified amount of uncompensated coverage has
been provided. - Fair Market Value: The value in arm’s-length transactions, consistent with the general market value (i.e.,
compensation that would be included in a service agreement as the result of bona fide bargaining between wellinformed
parties not otherwise in a position to generate business for one another at the time of the agreement). - General ED Call: Call coverage provided for general ED services.
- Restricted Call: Physician must remain on the premises for duration of call coverage shift.
- Telephonic Call: Compensation to treating physicians for providing telephonic consultations with no immediate
obligation to present to the hospital. - Trauma Call Coverage: Call coverage provided for trauma services only.
- Unrestricted Call: Physician is not required to remain on the premises but must respond to calls within a specified
time frame.
As health care reimbursement shifts from volume- to value-based patient-focused care, new models of compensation are emerging for physicians and advanced practice clinicians. SullivanCotter specializes in working with health care organizations to align physician recruitment, retention and productivity strategies with quality outcomes, patient satisfaction and efficiency through effective compensation approaches. We know the physician labor market as well as compensation and benefits trends and we understand the need to compete for medical talent.
In its ninth year, SullivanCotter’s 2013 Physician On-Call Pay Survey delivers comprehensive benchmarking data detailing on-call pay rates for more than 130 organizations and more than 40 physician and advanced practice clinician specialties, including more than 1,300 individual call panels. This annual survey is the only one of its kind that reports rates by physician specialty and type of on-call pay.